 Online training login
Online training login 
Over the past year we have been funded by the Scottish Government to develop a Talking Mat to enable adults with Learning disabilities to raise issues of concern. We have worked in close partnership with Survivor Scotland and Kingdom Abuse Survivors Project . Together we have developed and trialled a Talking Mat . The final report for this project is here :Talking Mats and Survivor Scotland final Report
This year the Scottish Government recognised the value of using Talking Mats as a conversation framework to enable people with learning disability to reflect on their lives and express their views including raising any areas of concern. One of the key themes from the national Scottish strategy for people with learning difficulties ‘Keys to Life’ is to keep people safe, but it was also recognised that the Talking Mat that had been designed could also help with other themes –
- Helping people with learning disabilities stay in control
- Shift the culture and ensure care is genuinely person centred
- Evidence that the views of people with learning disabilities have been taken into account
- Support people to cope with adversity and loss and enhance resilience
- Address health inequalities and reduce early deaths
The Scottish Government has funded a 3 year project which we are calling Keeping Safe.
This project will
- Produce a new resource based on the feedback from earlier projects This has 3 topics of conversation . Firstly ,How people are feeling about their Health and well-being secondly, their relationships. For people who are able to think and express their views at a more abstract level the resource has a third topic and gives them space to reflect on their thoughts and feelings.

- Train staff in the 14 health boards across Scotland to use Talking Mats and this resource specifically. This training will be provided jointly with KASP so staff can be supported to think through how they respond appropriately to any concerns that may arise
- Ensure that all health board areas have accredited trainers who will be able to lead ongoing training and sustain use of the resource
If you work with adults with learning disabilities in Scotland and would be like to be part of this exciting initiative please contact us at info@talkingmats.com.
Thanks to an OT colleague for this powerful story of how Talking Mats helped a woman with Multiple Sclerosis with goal setting by getting to the root of the problems she was having.
I am an OT working in a community rehabilitation team in Scotland. I have been seeing a woman (who I will call Jill) with MS. Jill has been experiencing increasing problems associated with her MS and finding it difficult to cope. During my first visit, Jill found it difficult to tell me about the problems she had been experiencing, and almost impossible to consider how we could translate these problems into tangible goals that we could work on. She was closed to any suggestions I made about potential rehabilitation goals. In her mind, the problems she had were there to stay, nothing could be done about them and she would just have to struggle on. We didn’t seem to be getting anywhere just talking about it. Jill was getting a bit exasperated and I was finding it difficult to keep a structure to our conversation and steer it towards agreeing on a goal that we could work towards. I felt there was a real risk of her disengaging from the service because we could not agree on a way forward.
Then I decided to use Talking Mats to see if that would help. I knew that using Talking Mats could help people with cognitive problems as well as those with communication difficulties. I wondered if doing a general Talking Mat using the Health and Well-being TOPIC symbols would help me identify what Jill thought her main problem areas were. Then I planned to do a sub-mat to look at her priority areas in more detail. My aim was to try and identify one or two rehabilitation goals (reflecting Jill’s priorities) that we could work towards. I really felt that there was potential to make a positive impact on Jill’s quality of life if I could get her to engage and agree on a goal to work towards.
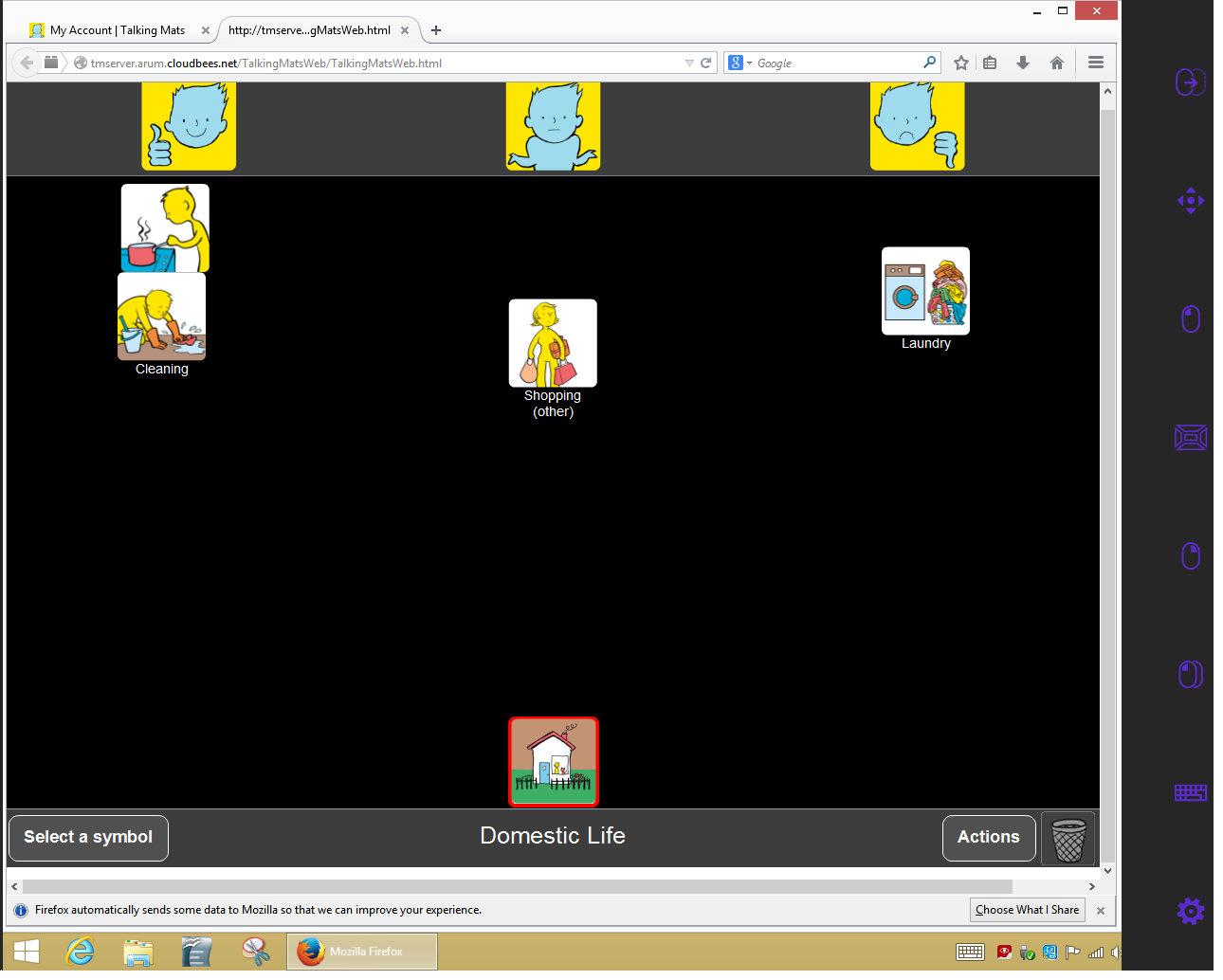
Using Talking Mats proved to be a great success. Jill very quickly got the concept of it. It seemed to be much easier for her to pick up a symbol card, consider it, and then place it on the Mat. Using the Mat appeared to reduce the ‘cognitive load’ of the conversation and gave her structure to work within which she found much easier. Jill was able to identify what her main problem areas/ priorities were: – Mobility and Learning/ Thinking (see picture of her Mat above). Jill was pleased that she had got her message across and actually seemed to enjoy the process of using Talking Mats.
Now we have got a starting point. In my next session I’m hoping to complete sub-Mats with Jill in the Topics of Mobility and Learning/Thinking. This will allow us to explore these areas in more detail. Using Talking Mats was a real breakthrough in Jill’s rehabilitation.
To read another blog about using Talking Mats with someone with Multiple Sclerosis click here
We are launching our fantastic eating and drinking resource to support shared decision making. This has been co-produced with the help of people with eating and drinking difficulties and a range of different professionals. The resource is designed to help people think about, discuss and make informed decisions about how to manage their eating and drinking more safely. People with eating and drinking difficulties should initially be assessed by a qualified Speech and Language Therapist and Dietitian who will recommend appropriate strategies to help them eat and drink safely. This resource is particularly useful in helping people understand the effect that their eating and drinking difficulties can have on their health. It also helps people talk about how they feel about recommended strategies.
When discussing eating and drinking, there are many issues to consider. We have provided symbols under three main topics to help present ideas in a structured way that reduces the likelihood that the person will be influenced.
Click on this image to see it more clearly.
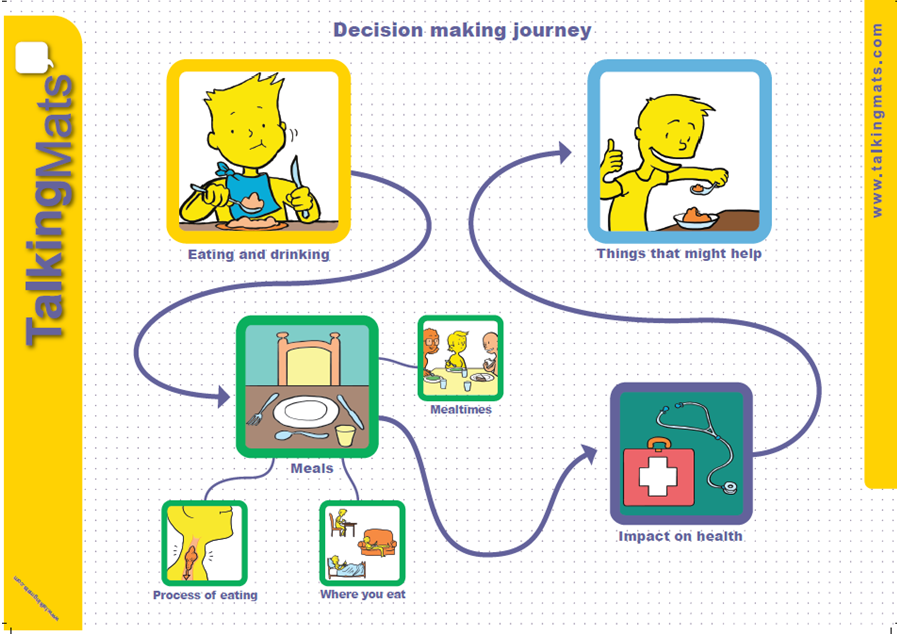
Discussing these topics separately means that people can firstly consider how they feel about different meal times, where they eat and types of food and then think about the impact that their eating and drinking has on their health. It also allows people to have a conversation about some of the suggested strategies and how acceptable these are.
Thanks to Lauren Pettit for this thought provoking blog about using Talking Mats in a rehabilitation setting in South Africa to compare goals of adults with aphasia, their Speech and Language Therapists and their significant others.
I am a Speech-Language Therapist in Johannesburg, South Africa and I work in neuro rehabilitation for people who have had a stroke or head injury. Over the past few years, I have been inspired to learn more about implementing communication modes to assist people to participate effectively in various communication interactions.
Talking Mats™ is such a wonderful tool that enables people to communicate so many things, from their needs and desires, to engaging in higher level conversations. I have seen the benefits of this tool used in a rehabilitative setting. I recently completed my dissertation with the Centre for Augmentative and Alternative Communication (CAAC) at the University of Pretoria, in South Africa.
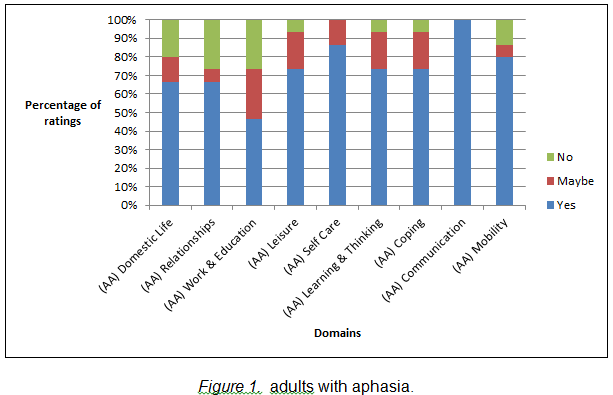
The study included adults with aphasia who were still attending therapy at least 6 months after their stroke and were working on activities and tasks in various therapies, for example: Occupational Therapy, Physiotherapy, Speech-Language Therapy, therapies. I wanted to understand what was important for them to work on in rehabilitation to improve in various areas of life. Some of the adults with aphasia had very little or no speech, others had difficulty expressing themselves and finding the appropriate words to use in a phrase or sentence. Talking Mats™ was therefore used to assist them to rate important life areas. The life areas (activities and participation domains) were identified by the International Classification of Functioning, Health and Disability (ICF). This classification system was created by the World Health Organisation (WHO) and may guide therapy assessment and management. The areas were depicted as symbols with a supplemented written word on each card. These nine cards were: Domestic Life, Relationships, Work and Education, Leisure or Spare time, Self Care, Learning and Thinking, Coping, Communication, and Mobility. The adults with aphasia were asked what was important to them to work on in rehabilitation. The adult with aphasia could place the card under Yes, Maybe or No on the velcro mat and provide a comment if he/she wished or was able to. The Speech-Language Therapists who worked with the adults with aphasia and their significant others (a family member/friend or carer, who knew the person well) were also included in the study. They were asked to identify which areas they thought were important for the adult with aphasia to still work on in therapy.
(Click on graphs to see clearly)
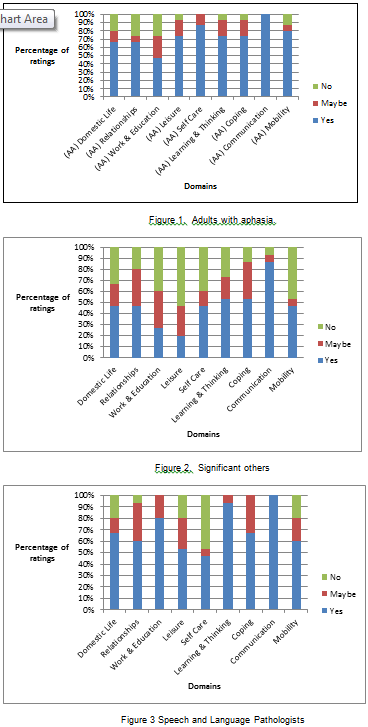
It was very interesting to see varied opinions in the results. Six of the areas received similar ratings from all the participants and Communication was highlighted as an important area to work on by all. There were statistical differences found for the following domains: Work and Education, Leisure or spare time and Self Care. The adults with aphasia wanted to work on Leisure or Spare time and Self Care, however, Work and Education was not important to them to work on in rehabilitation, whereas the Speech-Language Therapists rated Work and Education as important for the adults with aphasia to work on. Significant others did not rate these domains as important.
This study gave a glimpse into how some rehabilitation teams are currently communicating and working together and that very often, the people who have difficulties expressing themselves are perhaps not always given the time and space to understand the therapy plan and identify and communicate their individual therapy needs. This needs to be explored further. Talking Mats™ provided a structure and gave the adults with aphasia a ‘voice’ and the opportunity to engage in this complex communicative interaction. I am in the process of sharing the results from the study with the participants. I have encouraged them to sit together in their teams and identify areas that could currently be focussed on in their therapy. Many participants were eager to discuss the results after the interviews were conducted and were interested in the concept of prioritising their rehabilitation needs. I hope they see their participation in this study as the opportunity to further engage in their rehabilitation needs and that it gives them the confidence to participate more fully in many other areas of their lives that they identified as important.
I would so appreciate your thoughts and input. Please respond to Lauren lolpettit@gmail.com
We’re delighted that Andrea Powell, an Occupational therapist in Edinburgh has written a Blog for us about her experiences of being involved in group work with people who use AAC.
As a student occupational therapist, I worked part time as a support worker with an amazing lady Jennifer, (Jennifer is a pseudonym) Jennifer just happened to use an iPad to communicate. At this time I was about to commence my final year studies and was required to research and write a dissertation on a subject of interest. The lightning bolt of inspiration came when I, with Jennifer attended a weekly AAC user support group which was run and organised by a group of SLT’s.
The group was a wonderful resource that truly benefited the people who used it. I witnessed how much Jennifer valued spending time chatting with friends who also used an AAC device and who understood the unwritten rules of engagement. Such as patience while I set up my speech, don’t look at my screen while decide what I want to say etc. Her confidence in using different types of conversation grew while attending the group. It encouraged her to add to her already wide and variety vocabulary. As her support worker I also valued the opportunity to gain access to training on how to use her AAC and how I could provide better support to her.
I began reading around AAC and how people integrate of devices into their lives. I was however shocked to find that the wonderful group Jennifer attended was a rare occurrence for many users. The more I read, the more I realised that many users struggled to continue using an AAC device due to lack of support, access to trained professionals and most did not have wonderful resources like user support groups.
As an OT I was interested to explore the role in which I would play within AAC provision and found that as an OT I would be mainly providing support and advice on positioning, accessing devices and ergonomic type support.
However I felt that as an OT we have many more skills that didn’t appear to be to be getting utilised, within in my dissertation proposal I postulated that OT’s could expand their role within AAC to i) collaborating on assessments for AAC; ii) training on devices once they have been issued to users; and, iii) running and facilitating groups for AAC users and communications partners in the community.
OT’s are highly trained specialists skilled at understanding what is achievable and realistic for an individual. Occupational therapists assess individuals holistically in order to establish realistic and manageable goals which can be graded and adapted to suit the individual. Through the utilisation of appropriate grading of an occupation, a user can experience success and therefore less failure and frustration, ensuring the challenge is set at the appropriate level for the individual concerned (Park 2009).
Running and facilitating groups as a therapeutic tool is something that occupational therapists have been doing since the earliest days of the profession and groups are now utilised in many areas of practice (Howe and Schwartzberg 2001). By continuing this tradition, occupational therapists are well placed to take the lead in running and facilitating groups for AAC users, integrating social and community activities into the groups, for example, meeting in local shops to provide real life experience of interactions and, importantly, promoting the use of AAC to the general public. There are similar projects being attempted in Motherwell to increase the awareness of Dementia and make local businesses “Dementia friendly” (Shafii and Crockett 2013). Providing groups for AAC users not only enables them to learn how to use their devices, but also provides a support network of other users and communication partners.
I feel that if the skills of an OT were utilised in more than ergonomics then more positive outcomes could be seen for the user of AAC. I believe that if there were more OT’s taking on additional roles within AAC provision it could help reduce the pressure for SLT’s and the waiting lists to see SLT’s. It would also enable more users to be assessed to use AAC.
Thanks to Fiona Kane from the Alzheimer’s Resource Centre in Clydebank for sharing this lovely story about a visit to a man who had had a stroke. He was able to explain his views and take part in self management without realising it!
“Two of us visited a man who has aphasia. His wife is really struggling to communicate with him. She had been unable to attend the Talking Mats family training. I suggested the Talking Mats and they both agreed to try it out. I thought I would share it with you.
When we arrived the man was snoozing in the chair. He was extremely apprehensive when we first introduced the Talking Mats. However he quickly became very animated and we were able to tune into what he was saying.
A. asked him about gardening and he said he didn’t like gardening. He then invited us out to see his garden, was able to show us where he fell cutting a high hedge and indicated this was the reason why he had stopped working in the garden.
He told us he didn’t like religion and this was because his Mum was so strict with religion when he was younger.
He told us he really enjoyed photography and missed that. His wife is now going to buy a digital camera to help him continue with this.
He also told us that he enjoys listening to the radio but not radio 4 as there is no music.
His wife was absolutely amazed with the information her husband was able to communicate through the mats and he was able to express how much he enjoyed doing it. He was very animated and walked us out to the door.
It was a really amazing experience for both of us!”
Many thanks to Helen Paterson, one of our accredited trainers for this fascinating blog.
Now that Talking Mats is accessible in a digital format, the Talking Mats team are often asked ‘Can it be used on an eye gaze device?’ . Of course, for those who use eye pointing reliably, they can use a standard Talking Mat, but there are those individuals with whom we work with who may want to use their eye gaze device to use a Talking Mat, and who find the digital format more accessible. We would suggest that this is only done with a client who is already familiar with eye gaze , due to the extra effort required both to use eye gaze and to make decisions when using a mat. There are many other access methods with which you could use and access Talking Mats Pro, such as a head mouse, chin joystick or touch screen, but for this blog we will focus upon eye gaze. Here’s how we made it possible, and I am sure there may be other ways which we would love to hear about!
- To use Talking Mats Pro directly using eye gaze the person really needs to be calibrated on a device, and they require a level of calibration that is good enough that they are able to access a mouse emulator or Gaze selection on Tobii.
- You must ensure that the mouse emulation or Gaze selection features are set up and the person understands what the features are and what they mean e.g: left click, drag and double click.
- Open up Talking Mats pro on your account.
- You will need to select the topic, topscales and symbols for your client, as this will make it easier with less work for your client, although this is something you would do anyway as the person facilitating the mat.
- Now go through the question and the topscales as you usually would and explain them to your client.
- Select the first symbol and place it on the mat where they can see it.
This is where the 2 systems differ:
Mouse emulation: 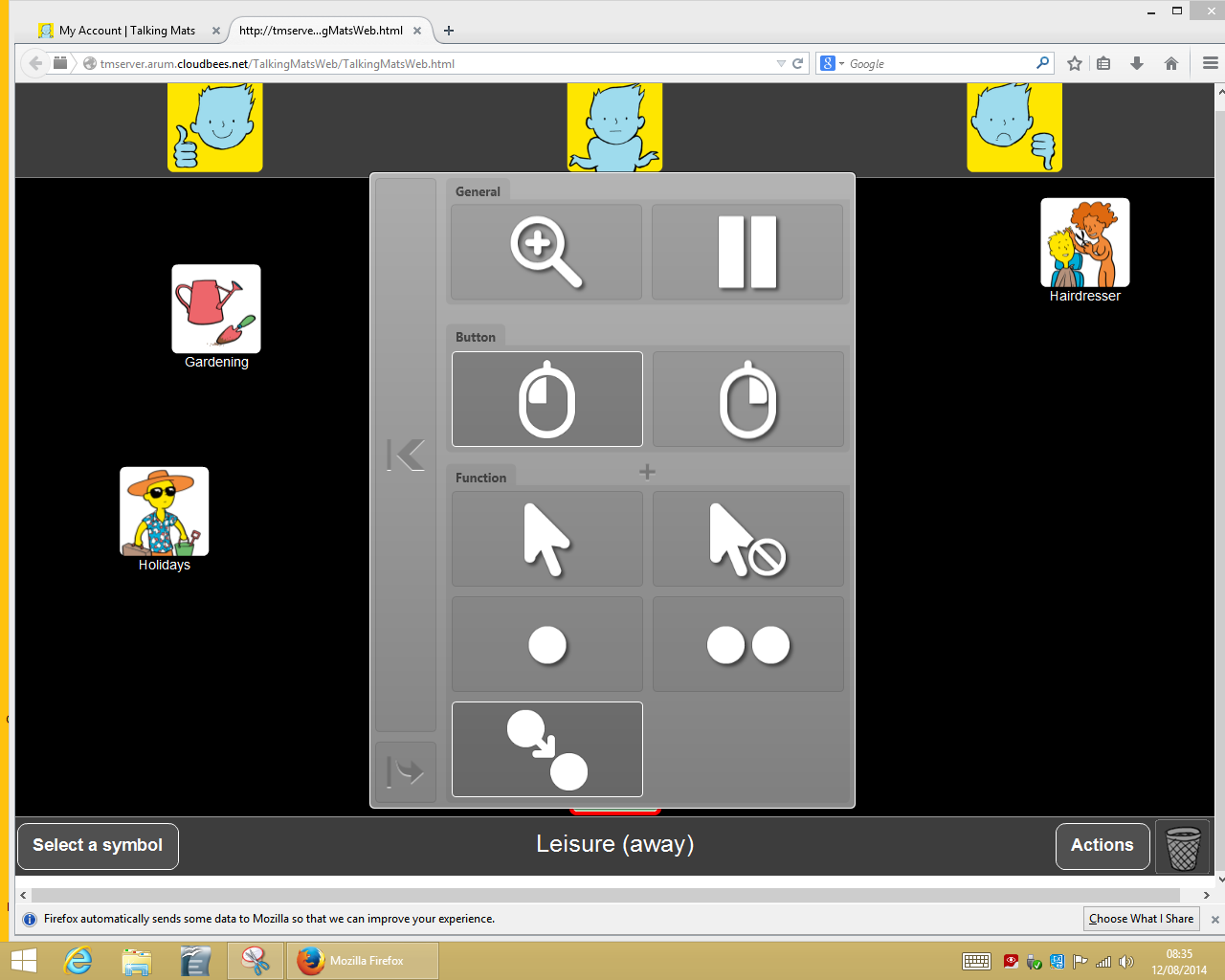 In mouse emulation mode, the user is emulating and controlling a mouse pointer on the screen. This function is available with software such as: Tobii Gaze Interaction in Mouse Emulation Mode (shown above), Alea Intelligaze, Eye Tribe with Dwell Clicker, Tellus 4 with TM4 eye tech, or the Windows App within the Sensory Software’s The Grid 2 FastTalker2 user.
In mouse emulation mode, the user is emulating and controlling a mouse pointer on the screen. This function is available with software such as: Tobii Gaze Interaction in Mouse Emulation Mode (shown above), Alea Intelligaze, Eye Tribe with Dwell Clicker, Tellus 4 with TM4 eye tech, or the Windows App within the Sensory Software’s The Grid 2 FastTalker2 user.
- Client first needs to open the mouse function menu by fixing his or her gaze on the small grey icon which will open the mouse menu.
- Client then fixates gaze to select the drag function (shown above)
- Then the client will select the symbol s/he wants to move by fixating on it.
- Once fixated, they symbol will ‘drag’ around the screen with the clients gaze. 5
- They will then fixate on a point to ‘drop’ it.
See Video
Gaze selection (Tobii):
 With Gaze selection (Tobii only) the user can control a Windows desktop with a two step selection method. The first step involves selecting the desired task from the taskbar on the right of the screen. The person looks at it until it changes to white. The person then looks at the part of the screen where they want the task to take place.
With Gaze selection (Tobii only) the user can control a Windows desktop with a two step selection method. The first step involves selecting the desired task from the taskbar on the right of the screen. The person looks at it until it changes to white. The person then looks at the part of the screen where they want the task to take place.
- The client clicks selects drag function at the top of the Menu
- They then look at the symbol 3
- They then look where they wish to place the symbol.
This does require some more thinking on the side of the client as they need to look to where they want it to go and they are not just dragging it as they are in mouse emulation mode.
See video
For individuals who do not have a calibration good enough to use mouse emulation or gaze selection, it is a little more complex. A Talking Mat could be emulated from software such as The Grid 2 or Communicator, but it would not involve the software from Talking Mats Pro or dragging of symbols and moving them to where the person wants them to go.
Thanks to Anita Devi,Education Consultant, for her helpful contribution to this blog.
The implementation of the recent SEND reforms in England requires interdisciplinary teamwork. Integrated assessments will now be carried out in cooperation with the young person and the parents. Capturing the child’s own perspective and recording their views, interests and aspirations is now a statutory requirement. The principles of the SEND Code of Practice state that practitioners should encourage the child or young person, and the child’s parents to participate as fully as possible in the decisions affecting their lives and use a common language to shape educational and other outcomes.
Talking Mats has produced a practical and creative resource – “Consulting Children & Young People” that helps practitioners to ensure that they take account of the SEND Principles at all stages of the assessment process and development of the EHC Plan.
We recognised the need to develop a tool that would give a holistic picture of how a child or young person feels about their lives at home, at school and in their communities. Having a visual framework means that there’s more time for reflection. You can help young people to see their personal strengths and abilities and take time to consider what their problem areas are. Talking Mats gives greater choice and control about what kind of intervention is required to support them.
Communication is a two way process and the role of the facilitator is crucial. Talking Mats provides training at the following levels:
- Awareness – an introduction to the Talking Mats framework and the development of the CCYP resource.
- Enhanced – a whole day training to equip practitioners to use Talking Mats
- Specialist – In depth training which allows the practitioner to train others in their organisation.
(as stipulated on page 58 of The 2014 SEND Code of Practice for England)
Why not sign up for one of our training courses and learn more about –
![]() Improving the quality of your engagement
Improving the quality of your engagement
![]() Creating a visual framework for consultation
Creating a visual framework for consultation
![]() A child centred approach to joint decision making.
A child centred approach to joint decision making.
Read Part 2 of this blog next week.
We are very grateful to Rhona Matthews for sending us this moving blog.
‘‘I met with Katie, the worker at Perth Young Carers who did the Talking Mats training and she told me this story:
It is recognised that there are many positive outcomes from being a carer.
For some young people helping care for a sibling can bring confidence, develop feelings of closeness to family and increase self esteem. However it can also add stresses and strains. Expressing frustrations or anger can be difficult and feel like a betrayal.
Using Talking Mats can make it easier to say the things that might cause upset. Using the Children and Young Person’s resource, a young person disclosed to a worker that the one aspect she was not happy about when helping look after her brother, was administering medication. She had seen this being done in hospital by injection and did not like the thought of having to do it. She was happy with all other aspects of helping with his care. The worker fed this back to her parents and they all agreed not to expect her to do this.
The worker felt that this issue would not have been highlighted without the Talking Mats.”
Angela is a speech and language therapist in Northern Ireland where she works with people with learning disabilities. She worked with John who had some difficulties with eating and drinking. Together they used Talking Mats to help John understand his risk of choking and identify foods which were easy or difficult to eat. Watch this film clip where John describes how Talking Mats helped him to understand and manage his risk of choking.



{kind=link}