 Online training login
Online training login 
When people have been in hospital for a period of time, for whatever reason, consideration needs to be given to discharge planning. There are often concerns about what a person may manage to do independently when they get home, and this often has an impact on where people are discharged to and what type of support they might need.
The ‘looking after yourself’ symbol sets in the health and well-being resource provide a good starting point for exploring some of these issues. This set is made up of three topic sets:
- Domestic life
- Self-care
- Work/education
I used these when I worked with a woman (Ruby) who had severe receptive and expressive aphasia. She had been discharged from hospital with a care package (carers came in three times a day to help her with personal care, meal time preparation and housework). Ruby had difficulty communicating through speech but was able to use Talking Mats effectively to express her views. I used the ‘domestic life’ symbols to find out how Ruby felt about managing the daily running of the household. Ruby was able to tell me that she felt she could now do more things around the house, such as hoovering and the laundry. She was ‘unsure’ about cooking and shopping, but indicated that these were areas that she wanted to work on.
Using Talking Mats, Ruby was able to tell me that she wanted to try to do more things for herself. We used photographs of the completed mats to discuss these issues in more detail with Ruby’s social worker and her husband. Initially, Ruby’s husband was hesitant about her doing more things around the house, but seeing the mat in front of him meant that he really listened to her views and felt happier about her taking risks and trying things for herself. As a result of our discussions, Ruby’s social worker reviewed her care package. She reduced the daily visits by carers and Ruby was given support from the rehabilitation team to help her work on preparing meals. Her husband arranged for a friend to take her to the supermarket once a week so that she felt more in control of the cooking. Use of Talking Mats meant that Ruby was really involved in setting her rehabilitation goals and ensured that her views were heard when her care package was reviewed.
The ‘looking after yourself’ symbols can be used to include people with communication difficulties in the decision making process. This is particularly important given the current legislative drive to promote self-directed support. Find out more about how to use Talking Mats by signing up for a training course at Talking Mats.
In a previous Blog, Joan talked about the four purposes of communication (Light 1988):
1. Expression of needs and wants
2. Information transfer
3. Social closeness
4. Social etiquette
Social closeness can often be overlooked when we support people with communication difficulties, as there can be a temptation to focus on what some see as the ‘important things’ – helping people to express their needs and wants or to transfer information. Social closeness is the glue which binds us together and helps us to form and maintain relationships. It’s really important that we establish this before we start exploring some of the difficult issues that many of the people we are working with face. In my work with people with severe aphasia, I spend time getting to know what matters to them and finding out what their interests are. This is a crucial part of building a relationship with the person and their family. It also provides a much more concrete starting point for beginning to explore rehabilitation goals, as this example shows:
When working with Jack (a man with severe receptive and expressive aphasia), I started by using Talking Mats to ask him how he felt about leisure activities. This was a great way to get to know Jack as a person and to find out his interests. During our conversation, Jack told me that he enjoyed going out for a drink but hated shopping and bingo – and we all had a laugh as he told me this. Jack also told me that he used to like ten pin bowling. He pointed to his leg to indicate that this was something he could no longer participate in as he was now in a wheelchair. I could see that this was important to Jack, so we talked about possible ways round his physical difficulties. Jack agreed that this was something he could work on with the help of his family and the rehabilitation team.
Given that Jack had severe receptive aphasia, if I had started by using Talking Mats to identify specific problems (using a top scale of ‘managing’ and ‘not managing’) as part of the goal setting process, it is highly likely that Jack would have found this too abstract and difficult to engage in. By using the more concrete topic of leisure (with a top scale of ‘like’/’dislike’), Jack was able to reflect on his life since his stroke and tell me how he felt about his restricted physical abilities. I was also able to build up a picture of him as a person and we had fun at the same time.
When using the Health and well-being resource, think about the person you are working with in relation to the ideas and concepts that they can cope with. Exploring leisure activities is a great way to start as it means you can establish rapport by finding out what matters to them.
Have a look at this Blog to see how other people have used a topic such as leisure to build social closeness.
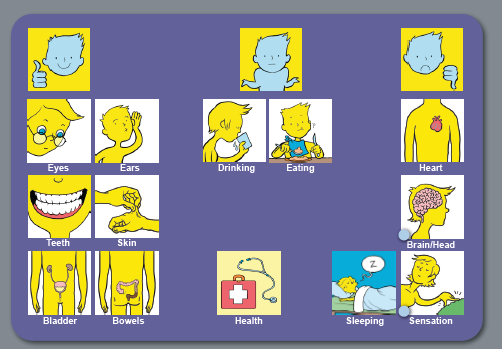
The Health and Well-being resource is based on the WHO International Classification of Functioning, Disability and Health (ICF) which is a framework which covers almost every aspect of daily life and can be applied over different cultures (WHO 2001).
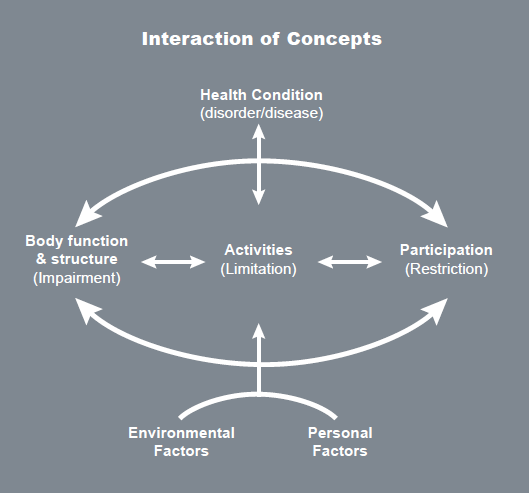
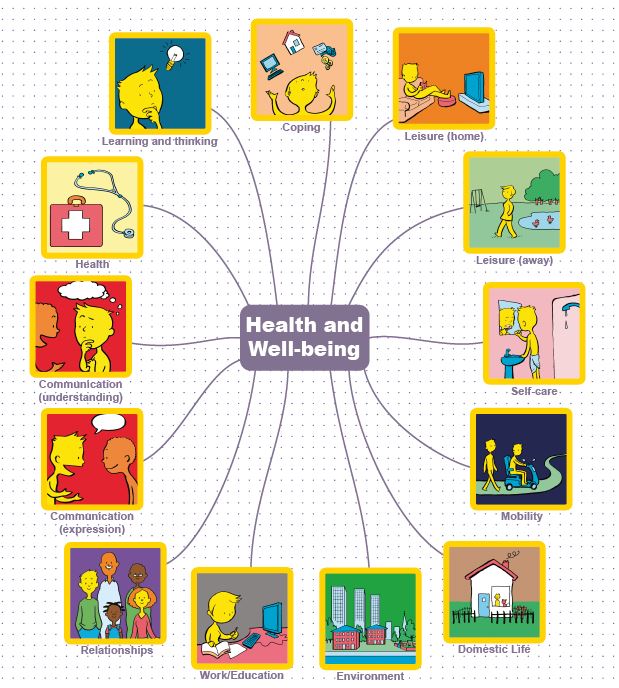
Use of the WHO ICF helps professionals to think holistically about the people they are working with. We have produced four sets of symbols, based on WHO ICF, to help people express their views about different aspects of their lives. These cover 13 topics:
You can use the symbols in different ways, depending on the cognitive abilities of the person you are working with. For example, if you are working with someone who can understand abstract concepts, you could start with the 13 main health and well-being symbols. Your top scale might be ‘managing’ and ‘not managing’. Here is an example of a mat completed by Duncan who had a stroke which affected his ability to communicate through speech:

Using these symbols as a starting point, Duncan could tell us that his main concerns related to worries about his health, expressive communication and work. From here, we did ‘sub mats’ to help Duncan identify the specific areas he wanted to work on/explore.
Here is the mat Duncan completed in relation to his health:
Having done this mat with Duncan, it became clear that he was worried about various aspects of his health, particularly the risk of having another stroke. The wider team were able to give him and his wife information about stroke prevention. Other mats were also completed, exploring expressive communication, work and education and higher level communication (which is included in the ‘learning and thinking’ topic, and covers written communication as well as memory and concentration). Using the Health and Well-being symbols, we were able to work with Duncan to help him identify the main issues that he wanted to work on and then work towards more specific rehabilitation goals. Duncan had copies of all the mats he had completed and found it useful to refer to them over the months. This helped everybody stay on track in relation to his goals and he was also able to track his progress over time.
Have a look at our Health and Well-being resource on our website. It is available both as an original Talking Mat with a physical mat and symbol cards or as a digital version as part of The Talking Mats pro subscription
Has Talking Mats been used in court ?
This is a question that we have often been asked and up until now we have been until able to give examples. On a recent training in Belfast there were two registered intermediaries, their role is to assist vulnerable witnesses and defendants with communication difficulties in the criminal justice system. The registered intermediaries scheme was set up in England and Wales and more recently was established in Northern Ireland. On the course they talked about two cases where Talking Mats was used as part of the achieving best evidence (ABE) interviews.
1. The first case was the case of R versus James Michael Watts http://www.bailii.org/ew/cases/EWCA/Crim/2010/1824.html . Here the clinical forensic psychologist used them to support an individual with severe disabilities to express her view of what had happened.
2. The second case that was discussed was the work of a registered intermediary, Catherine ‘O’Neil where she used them with a young man called Tim in his early twenties who had been severely stabbed and suffered a severe head injury which resulted in locked in syndrome. He had some very limited movement of his hand. Initially, Catherine worked with him to establish a yes/ no and then went on to assess Tim’s ability to use Talking Mats. The focus of the first Talking Mat was to find out about his interests and to enable Catherine and Tim to engage and interact with each other. Catherine said ‘he seemed totally relieved to be able to communicate his narrative. This allowed us to get to know him and his likes, dislikes and interests. Tim had never been a great friend of the police and in the like/dislikes/ don’t know mat, I included many pictures including Basketball, which went slowly but immediately to YES; Snakes under No and Police he joked and eye pointed to the door.!’ Catherine went on to use Talking Mats and these were used jointly with the police in 5 ABE interviews. This did enable evidence to be gathered in terms of the assault weapon, people etc. Through the support of a skilled registered intermediary Talking Mats contributed to enabling the victim to have a voice at the trial where otherwise none would be had. In this case a conviction was made.
We like to keep up to date about how Talking Mats is being used. You may well know of other cases where Talking Mats is being used to support people with communication disability to access justice. If so we would love to hear about them so please let us know.
The final part of my keynote talk at the AAC Conference in Helsinki last month focused on what we mean by communication effectiveness.
It is important to be able to determine the effectiveness / success of an interaction between two people, whether they are politicians, parent and child, husband and wife….. people using AAC systems or people using their own speech.
When I carried out a literature search of peer reviewed journals for my PhD in 2009 I could find no clear definition of communication effectiveness. Some people thought that effectiveness was synonymous with ‘word intelligibility’ or ‘correct syntax’. Others defined effectiveness in terms of the number of words produced on an AAC device. One publication even suggested that effectiveness was demonstrated by someone taking responsibility for charging their AAC device!
The main focus of all the papers I found, which mentioned communication effectiveness, was on needs and wants and only 3 papers cited social closeness as important (click here to read previous blog).
However, some publications did give useful pointers. Light (1988) emphasised that effective communication depends on 2 way interaction and that the partner is a major factor in the success or failure of communicative interactions. Lund (2006) described adequacy, relevance, promptness and communication sharing as key indicators. Ho et al (2005) highlighted satisfaction – partners’ feeling of how well they communicated during the conversation. Locke (1998) stressed that determining the success of any communication is a subjective undertaking as ‘Communication is not a mathematical formula of phonemes, morphemes and syntax, but rather includes casual conversation such as gossip’.
The Talking Mats team has tried to capture what we believe are the essential factors in determining communication effectiveness. We have produced a simple tool – the Effectiveness Framework of Functional Communication (EFFC) which can be used to chart key factors in an interaction on a 5 point scale and give an overall indication of whether the conversation is effective or not.
We have used the EFFC in several of our research projects and show participants how to use it during our training workshops. In Finland I tried it out with the audience of 200 AAC professionals using 3 video examples of different AAC conversations. The resulting scores were amazingly in agreement suggesting that this is a reliable tool.
For a free download please click here EFFC 2014
We would welcome any comments or questions.
In my last blog I wrote about the purposes of human communication and suggested that social closeness is essential for effective communication. Janice Light, in her 1988 model, described social etiquette as the ability to conform to social conventions of politeness and one of the key purposes of communication.
I believe that social etiquette has been overlooked when working with people with communication difficulties. Social etiquette may be seen as ‘the cherry on the cake’ and not really necessary, when getting a basic message across is so difficult for someone with a communication disability. However, the way in which someone greets you when they meet you, how they show interest in what you are saying or how they say goodbye, all effect how you respond to them and can influence your subsequent interactions with them.
Moreover social etiquette can often be done non-verbally – a smile to show you are pleased to see someone, a nod of agreement to show you are following what they say, a handshake or ‘thanks for coming’/’good to talk to you’ when you say goodbye. These are all basic and almost universal communication symbols.

Social etiquette is not just a communication add-on that can be missed out because it’s too much effort. It can be crucial in developing and maintaining relationships.
Not many people enjoy going to the dentist but it can be a real problem for people with communication disabilities.
Recently I wrote about using Talking Mats in a care home to find out the views of an elderly lady with communication difficulties and dementia who had lost her dentures. click here. Using the mats, she was able to tell us that she was unwilling to open her mouth but thought that if someone was with her she might manage better.
Following our Talking Mats conversation the Care Home arranged an appointment with the dentist for the following week. Her son went back over what we had talked about just before the visit. She managed fine, opened her mouth and her treatment was carried out successfully.
 Her new dentures are on the way!
Her new dentures are on the way!
Dentistry is a huge problem for many people, but the impact of not being able to cooperate can have serious implications for a person’s appearance, comfort, quality of life and health.
In preparing for a visit to the dentist it’s important that the person understands both what is going to happen and why its happening. Talking Mats is a visual tool that can help the person with communication difficulties both with understanding and also expressing their views. In this way the family and carers can find ways to reassure the person and support them to get the appropriate dental treatment.
Please let us know your thoughts on supporting people in similar situations.
The Talking Mats Team is increasingly asked to help ascertain a person’s capacity to express their views from a non-biased perspective. We are also asked to carry out service evaluations and are therefore developing independent consultancies to individuals and organisations. Our team of experienced Speech and Language Therapists, who have an in-depth knowledge of communication difficulties, are well equipped to do this.
The following are examples of independent consultancies which we have been asked to carry out:
- A lawyer asked us to work with a man who had had a severe stroke to ascertain his capacity to make decisions ranging from simple ones such as where he would like to go on holiday to complex ones such as who should control his finances. Using Talking Mats we were able to determine that he could make decisions about simple, concrete situations but wished his wife to make more complex decisions such as finances. check
- A Social Work department asked us to work with a woman with dementia and aphasia who had been sectioned. They needed to ascertain if she could understand why she could no longer live in her own home. We worked closely with her social worker and through using Talking Mats ascertained that she was unable to give informed consent.
- A Health Service facility asked us to evaluate the degree to which their patients felt involved in their care planning.
- A Care Home asked us to use Talking Mats with a 91 year old resident with dementia to find out her views about receiving dental treatment. There had been problems in the past and both the staff and her son were unsure if she understood the reasons and implications for dental treatment. Using Talking Mats, she was able to explain her thoughts about her teeth and dentures and clearly said that she was unhappy about opening her mouth for the dentist but that if her son were with her she would feel much better. We received this comment: “If you were to show the first few minutes without Talking Mats you would have thought this lovely lady lacked capacity, however the change and her engagement is noticeable.”
The following points explain with whom and how we can carry out the Talking Mats consultancy:
- Children or adults
- Family members, friends, professional staff
- Individuals or groups
- With or without a carer present
- At a venue and time which best suits the individual
- On any topic – we already have a comprehensive range of topics for both adults and children – but can create tailored symbol sets for any situation
- To find out someone’s views on a particular topic or situation at a specific point in time
- To help determine the capacity of an individual to make their own decisions
- To compare someone’s views over time
- To compare different people’s views e.g child and parent, person with dementia and carer
- We provide a detailed report with a copy of the person’s completed mat/s
To find out how we can help you and for discussion of costs please contact us at info@talkingmats.com or phone us at 01786 479511
“About half of all people with multiple sclerosis have some degree of problem at some time with aspects of thinking – memory, attention span or concentration. …. Many people may not recognise cognitive symptoms as an aspect of their MS and they can arise early in the course of the condition although the greater the disease duration and severity the more likely problems are to occur”. MS Trust
Talking Mats is one tool which can help people recognise any problems they may be having. It also provides a sensitive way for people to discuss these issues and plan ways to manage their situation.
We have developed a range of topics which encompass virtually all aspects of a person’s life
Insert mind map
The Learning and Thinking topic is particularly relevant. The following is an example of a Talking Mat done with Stella who has MS and lives at home with her husband and 3 children.
Top Scale Used: Managing: Need some help: Not managing

Stella began by putting most of the option symbols between the Managing and Need some help columns. However as more symbols were presented, she took time and thought about each symbol more carefully and changed her mind about many of them.
She said that using Talking Mats helped her realise that she was having some problems. On completion of the mat, she showed it to her husband and together they discussed practical ways of ways of managing her difficulties.
There are a further 12 topics in the Health and Well-being resource that can be helpful to people with MS. these are available either on our app or as Talking Mats original.
I undertook the ‘Talking Mats’ on-line course to acquire a new skill and a way to enhance my communication with people with dementia in practice. I have found the learning strategies used are varied and interactive – so there is not a sense of sameness, even though visually there is a consistent layout to the presentation of each module (this expedites navigation). This enhances engagement and my interest so that I am never reticent in logging on to complete the next module! In the beginning, I felt that I could move a lot quicker through the course if the modules were available once each part was completed, instead of having to wait for feedback on each assignment. However, nearing the end of the training course, the benefits of this approach are now clearer. Spaced learning and spaced practice allows for thinking time and internalisation of the module components. In this way, I have come to appreciate the part skills involved in the overall process and how they come together. I now find myself observing the skills involved and the reactions of all communicating as well as the surrounding environment, body language etc. I have also found myself looking back over the past module materials to ensure I am integrating as I go and to remind myself of the rationales for the actions that need to be taken, as well as ensuring that I am more and more familiar with the new terminology that I have been exposed too.
Little did I know when I signed up that the benefits of learning about and how to use ‘Talking Mats’ would stretch wider than what I initially anticipated or wanted! In completing the course, I am now much more aware of my communication practice in general, and the part-skills involved. I can also now see the wide applicability of ‘Talking Mats’ to different populations, age groups and conditions. Communication is everywhere but it needs to be efficient and effective – I am now more confident that my communication practice will improve as a result of this course. For me this is the best outcome possible.
Please click here to find out how to book on the next course


