 Online training login
Online training login 
This year, we wanted to give you plenty of notice of our upcoming January 2024 sale!

You can expect 15% off selected resources from the 1st -31st January 2024. These include:
Advanced Resources:
- Eating and Drinking
- Thinking Ahead
- Keeping Safe
which were £55.00 each and now £46.75 each plus postage and VAT.
Post Training Resources:
- Youth Justice
- Social Care
- Careers, Work and Employment
were £38.00 each now £32.30 each plus postage and VAT.

We also have 50% off Leisure Conversation Sets.
- Leisure Subset: Sport was £38.00 plus postage now £19.00 plus postage and VAT.
- Leisure Subset: Out & About was £38.00 plus postage now £19.00 plus postage and VAT.
All sale items will be automatically discounted between the 1st – 31st of January 2024.
Visit www.talkingmats.com/shop.
Merry Christmas and a Happy New Year from the Talking Mats Team!
Postage starts from £6.50 (plus VAT). All orders must be placed before the 31st of January 2024.
For organisations paying by Purchase Order, payment must be received within 28 days of the date that the order is placed for price to be guaranteed. Please make sure to include the £6.50 (plus VAT) postage cost on your purchase order document. If you require a quote for the purchase order, please email finance@talkingmats.com.
Walking Back to Happiness.
We may not be able to guarantee happiness but our friend and advocate, Karen Mellon is running a further training on our Foot Care resource and that is definitely something to sing about!
Developed late 2021 and launched in 2022 the Foundation Training with the Foot Care resource was so popular we are running it again. The resource was developed in collaboration with Karen and her team at NHS Fife Podiatry but it is aimed at anyone for whom footcare is part of their role. The College of Podiatry recently published figures on costs to the NHS in England and diabetic foot care alone cost £1 – £1.2billion per year. Supporting patients to communicate health issues around their feet is one step towards ensuring they access the right care at the right time.
Karen recently presented to the Allied Health Professional’s Dementia webinar describing the resource from development to practise. You can view the presentation here, and read her blog from 2021 here.
The training is delivered on Teams in 2 sessions – January 24th 2024 and February 21st. Both sessions run from 9.20am – 12.30pm and both must be attended. The cost is £210 and this includes a copy of the Foot Care resource.
In the first of a 2 part blog Larissa, our new Intern, introduces herself and our new Youth Justice Resource and gives information on a Talking Mats seminar at the end of April to mark the launch.
Hello!
My name is Larissa, I am a fourth year Psychology bachelors’ student at the university of Stirling and currently working on the launch of the Youth Justice Resource with Talking Mats as part of my work placement this year. Having enjoyed studying modules such as Language and the Brain and Developmental Psychology at university, I find the products Talking Mats have developed fascinating and love reading about in which ways the mats have helped people communicate in different situations.
I believe by adding the mats into any conversation -and especially around difficult or abstract topics- it can really open a two-way street of conversation. Instead of a person feeling they are being talked to, they are being asked to join the conversation, interact and show using the mats what they think. This can be beneficial for users who experience difficulty around communicating but also offer structure to any kind of conversation.
Especially in the context of Youth Justice I think this will be useful as having conversations about topics linked to a young person’s behaviour is fundamental to delivering appropriate and effective care. Conversations about difficulty in one’s personal life can be quite challenging. There are often delicate topics, the person might feel ashamed or find it hard to put into words what they have experienced or what they are feeling. This is where the use of Talking Mats can offer a less threatening way to broach a variety of topics and provide a structure to support conversation
The symbols in this set will help users communicate their experiences and how they feel about relationships, places and spaces and their experience with Youth Justice and was developed with a Youth Justice setting in mind. However, there is clearly a much wider use for this resource in any setting where understanding a person’s behaviour based on their experience and feelings is vital to determining the best form of support.
So, save the date! To celebrate the launch of this new set Talking Mats is having a web-seminar on the 28th of April 2022 at 9:30am after which the resource launches on the website. Come along to find out all about this new set, its uses and how it has helped Justice Practitioners so far. We would like to invite everyone who is interested to sign up on Eventbrite following this link:
Furthermore, please feel free to get in contact with us should you have any questions.
Manchester 30th June 2022.
It has been a long time since our Associates have been able to deliver training in a venue that is not virtual (to be accurate usually their kitchen / bedroom / garden shed). We are really pleased, therefore, to be able to let you all know that face to face training has returned! We know the convenience of online suits some people but many of you have been really missing the interaction, the energy and the discussion that occurs in a face to face training and we are looking forward to getting back to working with you in the same room.
It will be held in the St. Thomas Centre, Manchester on the 30th of June from 9.30am until 4.30pm. Find out more about what to expect on this course by following this link Manchester June 2022.
Talking Mats will take every step required to keep all participants and staff safe in this situation. Please let us know if there is anything we can do to support you to attend this course.

This course will be run by Laura Holmes, Lead Associate with responsibility for Foundation Training. She has been training with us since 2016. Here are her thoughts on resuming face to face training;‘I get so much out of face to face training; particpants form relationships quickly and really respond to each other and it creates a special learning environment.’
There are only 12 places on this course and we expect them to be taken up quickly.
To book please follow this link BOOK HERE.
Our new digital platform with enhanced features
Talking mats have been researched and developed over a period of more than 20 years. Initially Talking Mats developed as a paper based communication framework but there was always much interest in having it as a digital resource so our first digital Talking Mats platform was released in 2012.
In the years since its release the Talking Mats digital platform has helped thousands of people who otherwise would find it challenging to express how they feel, but with the discontinuation of Flash player the opportunity to create a new web-app presented itself. We are delighted to say that it is here! Combining it with the new website means that we are able to include many of the features that our customers have wanted, including the ability to:
- Add and save photos
- Personalise conversations by adding symbols from other sets
- Create and save your own personalised mats ( provided you are foundation trained )
- Think through and order your Talking Mats conversation
- Change and select an appropriate Top Scale
- File your thinker’s mat in an easy to retrieve manner
- Easily carry out remote Talking Mats conversations
In a nutshell
The new Digital Talking Mats (DTM) is a subscription-based web app which is access via our new look website www.talkingmats.com. It contains all the Talking Mats resources currently available to purchase to ensure that it can be used in as many different contexts to help as many different people as possible.
The subscriptions
We wanted to ensure that there was a DTM subscription for everyone. To that end, there are three different levels of individual subscription (starter, enhanced, complete) which can be renewed on a monthly or annual basis. There is also a licence specifically for organisations which offers the chance to have multiple users tied to an organisation, all at ‘complete’ level.

Once you have signed up for a subscription, you can easily see the details in the ‘subscriptions’ section of your account.
App Features and How to Use Them
Once you have subscribed and accessed the app, there is immediately a helpful video which tells you all you need to know about how to use the app. This includes setting up a new thinker, creating a new Talking Mat with the symbols of your choice, and how to view snapshots of previous sessions you have carried out.

Technical Tips
Browsers
All browsers are equal, but some are more equal than others. Our app is optimised for Google Chrome, but will also work on Firefox and Microsoft Edge. Internet explorer is not supported. It is a good idea to make sure your browser is as up to date as possible for the best user experience. More detailed information on browser compatibility is available here
Offline Functionality
We recognise that internet is not always available in homes, schools or many other places, and so it is very important to us that the app works offline. Unfortunately due to the fact it is till relatively fresh, the app will not work offline yet, but rest assured this feature is in the pipeline. One option in the meantime is to use a device that can hotspot (most smartphones will have this feature) and carry out a Talking Mat online.
App Navigation
When you are navigating from page to page in the app, it is actually creating overlays on a single web page. This means that when you are in the app, if you press the ‘back’ button on your browser, it will take you out of the app completely.
If you have any questions about the Digital Talking Mats platform or you are interested in learning more, you can get I touch with us at info@talkingmats.com.
On Wednesday November 10th we held a colloquium with the University of Edinburgh and NHS fife to report on the findings of the research that was funded with the Burdett foundation . The easy-read version of this report can be found here.
48 people attended the online event on Wednesday and engaged in some very thoughtful discussion and reflection on communication in forensic settings. There was much to think about including whether ethos and values align with self-determination , how to get communication taken seriously by staff who are often under huge pressure. Consideration of where power lies in an organisation and an acknowledgment that in order to share power staff themselves need to feel they have power.
The recognition that in the promotion of shared decision making, you increase the risk of people taking what others may see as unwise decisions. The need to support the capacity of people to be involved in decision making early on and in the smaller decisions of life and not leaving including them to a crisis.
The importance of further research in his area and that small clinically driven research projects have an important role to play in addition to ones funded by bigger grants. There is much to digest and we are hoping to keep the conversation going.
If you would like to see for yourself the research presented and the topics discussed at the colloquium you can watch the recording of the Zoom session here.
If you want to attend foundation Talking Mats training please find out more here. if you have completed your foundation training please consider attending the Keeping Safe advanced online module which includes the Keeping Safe resource . If you have the Keeping Safe resource please download the new Being Included bolt on to use with it.
We are all continuing to live in challenging times due to the COVID-19 pandemic, and there are concerns about the impact on the mental health of people at all ages and stages of life. This is a good time to reflect on the wide variety of blogs that have signposted how useful Talking Mats can be in helping people to think, structure coherent responses, and express their views. If this is an area of interest to you then take a look at these blogs to find out more:
- Debbie Mole, Clinical Nurse Consultant in Mental Health and Intellectual Disability for DHM Mental Health Care in Melbourne, Australia shares a great example of the positive impact Talking Mats can have for people who have experienced trauma. https://www.talkingmats.com/talking-mats-and-trauma-work/
- Natalie Paris, CashBack 180 Project Lead shares some powerful examples of how Talking Mats has helped her to open up conversations with the young people she works with https://www.talkingmats.com/opening-up-conversations-with-young-people/
- Edith Barrowcliffe from The Action Group demonstrates how Talking Mats has allowed individuals with intellectual disabilities access talking therapies and counselling. https://www.talkingmats.com/counselling-communication-1/
- Edith expands on this work in her second blog, describing how she adapted this approach to use during remote support during lockdown. https://www.talkingmats.com/counselling-learning-in-lockdown/
- Jo Brackley, NHS Clinical Lead for SLT Secure Services (Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust) describes how Talking Mats helps people with mental health open up and have richer conversations, with increased novel information gained. https://www.talkingmats.com/covid19_securehospitalsetting/
- Susan Gowland, SLT at NHS Fife Forensic Learning Disability Service, describes how Talking Mats support patients to express what they think in forensic learning disability setting. https://www.talkingmats.com/forensic_ld_setting/
- Dr Carla Innes, Clinical Psychologist for Learning Disabilities at Stockport Healthy Young Minds (CAMHS) describes how Talking Mats helps the team to gain more insight to the children and young people they are working with, and how it has helped intervention focus on the child’s potential, and zone of proximal development. https://www.talkingmats.com/talking-mats-and-mental-health/. This work in Stockport is further expanded on in a presentation by Dr Rosie Noyce, Clinical Psychologist, given at the Talking Mats 21st Birthday Event in August 2019. https://www.talkingmats.com/wp-content/uploads/2019/08/Talking-Mats-and-Young-Peoples-Mental-Health.pdf
- Georgia Bowker-Brady, Advanced Specialist SLT (Berkshire Healthcare Foundation Trust) describes how using Talking Mats in dementia care and acute health patient inpatient services helps patients organise their thoughts and express what is going well for them, as well as what isn’t. https://www.talkingmats.com/acute-mental-health/
- Rachel Woolcomb, Talking Mats OT Associate, explains why Talking Mats supports thinking, and why it can be particularly useful in helping people to structure and express their thoughts. https://www.talkingmats.com/talking-mats-as-a-thinking-tool/
We would love someone to carry out some research in this field, so if this sparks a research or blog idea, please get in touch with us at info@talkingmats.com.
Many thanks to Natalie Paris, CashBack 180 Project Lead for our latest guest blog. Natalie shares some powerful examples of how Talking Mats has helped her to open up conversations with the young people she works with:
I joined Y2K Mayfield and Easthouses Youth 2000 Project in February 2018 as a sessional worker looking to gain practical experience in youth work, I then became Part Time Young Women’s worker at Y2K, which gave me experience in working with vulnerable young women in Midlothian across an age range of 11 to 24, some with mild to moderate learning difficulties. When I first heard about the 180 project, I knew it was something I really wanted to be involved with, as I have always been interested in Criminology and Youth Offending.
In September 2018 I became the full-time 180 Project Lead, and have helped to shape and develop our CashBack 180 Project. CashBack 180 is a referral-based service, focusing on early support and prevention for young people involved in or at risk of becoming involved in offending, anti-social and risky behaviours.
The Project:
We work with young people to make positive changes in order to work towards more positive futures. Young people accessing this service have the opportunity to take part in fun, participative and educational programmes of activities as well as 1:1 supports. The CashBack180 programme is delivered at Y2K, but we can also deliver programmes within High Schools.
CashBack 180 offers a menu of options and has adapted where necessary for our journey through the pandemic.
- 1:1 supports
- Groupwork programmes
- Community outreach support through detached youth work
Case Example 1:
A 12-year-old girl had been referred to me for violence, as she had attacked a girl in the playground, which was out of character for her. She was very uncomfortable in the 1 to 1 session, so I used a Talking Mat. This made the conversation flow more naturally.
I used the Relationships topic, with the top scale ‘going well/okay/not going well’. This helped me get more information. I found out that most of the issues she was having were around peer relationships. For example, friends saying things that weren’t true, and not being believed by others in her friendship group. This allowed me to plan a session around what is healthy and unhealthy in friendships.

Case Example 2:
I was working with a 14-year-old care experienced boy, who had been referred to me for Anti-social behaviour, and because he was easily led. Once I got to know this boy a little better, I realised that he did not have much support within his family, apart from his older brother who he lives with now. I realised he was someone who had just learned to cope himself, and probably didn’t have many people to turn to when worried about things. I thought coping would be a good topic for a Talking Mat, as he always said things were fine, but I didn’t feel it was the full truth. I used the top scale ‘going well/okay/not going well’. This gave us the opportunity to discuss healthy and unhealthy coping mechanisms that he had and what he could do instead.
Case Example 3:
I was working with a 12-year-old care experienced boy, who had been referred to me due to his inappropriate sexualised language and reference to sexual experience. He has been out Mainstream school for 1 year, so had missed P7 sex education. I decided to start working on friendships and relationships over the first couple of weeks with him, to get an understanding of what he knew was acceptable in relationships. I used the Relationships Topic with the top scale ‘Going well/Okay/Not going well’. The Talking Mat helped me keep his attention for a little longer than usual, as he is a very chaotic young person and often gets up and walks about, or jumps on tables and pretends to be sleeping. It also showed me that he felt quite happy but was missing his friends from where he used to live. We are now looking at ways to address this.

Follow this link to Find out more about this project:
180 Service – Mayfield and Easthouses Youth 2000 Project
If you are feeling inspired and would like to know how you can access Talking Mats training, find out more here: https://www.talkingmats.com/training/
We are delighted to share this latest guest blog from Debbie Mole, Clinical Nurse Consultant in Mental Health and Intellectual Disability for DHM Mental Health Care in Melbourne, Australia. This is a great example of the positive impact Talking Mats can have for people who have experienced trauma.
Throughout my 35 year career I have always had a big interest in finding ways to help clients express themselves. My passion is around trauma and working in creative ways to help bring some closure and recovery for the person.
This desire grew when I met a woman who had multiple disabilities. She was blind, deaf, and non-verbal. She was sensitive to touch and had very few ways to express herself. She needed to be admitted to hospital as she was unwell, we had no way to explain to her what was happening. At the time I was working in a new specialised mental health and disability team. This humbling experience of working with her pathed a way for me to find ways to help people communicate and understand.
Working in mental health I am acutely aware of risks and that so many people who struggle to verbalise thoughts, feelings, and past issues. I was always concerned that because a person could not verbalise their thoughts, feelings, and intentions that so much information and potential risks were being missed.
I heard about Talking Mats training in Australia and booked myself on the course. This inspired me and has helped me support clients to find a voice and solutions to issues.
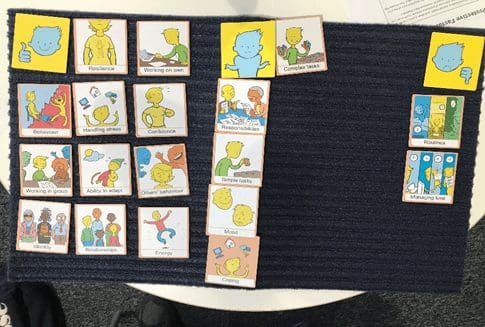
My client was a 30-year man with Down Syndrome, he also has ASD and over the last five years had lost his ability to speak. When I met him, he had poor eye contact and appeared to be locked into his world. It was evident he was also suffering from psychosis as he was responding to auditory and possibly visual hallucinations. He could use some sign language to communicate. He had chronic OCD and anxiety and sleep was a major issue.
I did a Talking Mat exercise and checked his understanding of “like”, “don’t like” and “not sure”. I did a simple exercise to start using the images for his family and carers. There was no real form and the cards appeared to become a collection of images that did not hold any clues.
I decided to use to the personal care cards, this was very different. Showering, bathing, and going to the toilet were placed in the negative area. There was also a change of behaviour and some vocalisation of words that made no sense. Talking to his team and mother, there was a restive quality to his behaviour – he wanted to avoid this area.
I did further assessments and his mom believed that in the past when he was young, he may have experienced some bullying, she also feared that he had suffered some form of abuse. Through the assessment it also transpired that my client was one of five children, all had a significant mental health issue. I organised a specialist to see him and he was diagnosed with Schizophrenia. He was treated with antipsychotic medication.
As the psychosis was being treated his team became aware that my client was starting to talk, it was not clear, but the content had a theme. Tragically themes, names and places started to be spoken about. When he spoke about these events his OCD behaviours of arranging his items on the floor became more chaotic. He spoke of trauma from other boys that took place in bathrooms.
I worked with the client and introduced some basic trauma work, simply allowing him to say what he wanted to and then helping him to realise that he was safe and that was the past. His team did the same. We offered choice about showering, bathing and looked at ways it could be fun or a nice activity to follow. The idea was to change his thinking around baths and showers and for him to realise he was safe and free from threat. We used the talking mats to build upon the things he liked.
I repeated the Talking Mats exercises three, six, nine and twelve months after treatment.
After the psychosis was treated, we became aware that the client looked sad and flat. There was a loss of interest in social activities and there was a lot of talk about the past. We assessed that he was depressed and that it was possible that his recall about the past was becoming clearer. He was commenced on an antidepressant and monitored intensely. We also needed to address the sleep issues. His OCD had led to his bed to being covered in items. We later realised that this helped reduce his anxiety when he was heightened.
My client has regained some speech, I believe he was locked in a world of trauma and psychosis. Now he mentions the names of some of the people who have hurt him. His team reassure him that he is safe, that was the past, and he is ok. He seeks physical attention when he distressed, and he is acknowledged and reassured. We cannot offer typical trauma therapy to him, but just helping him unlock his thoughts, knowing that what was happened was wrong and being heard is healing.
I have since developed my own set of cards, based on the Mental State Examination. I use these to expand on issues and focus on problem areas. These cards talk about perceptual issues, thought problems, beliefs and risks, all areas that are typically private and too often unexplored. The cards have images on them, so clients who struggle to verbalise can use the same system as the talking mats.
Talking Mats allowed me and his team to see things from a different angle. There were many hypotheses used to gain an understanding of his behaviour. This led to effective treatment and partial recovery.
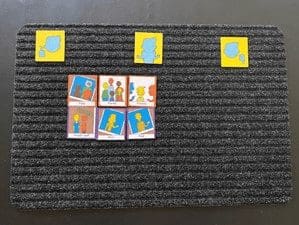
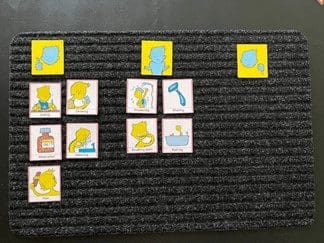
Picture 1 at the assessment stage, images of the clients family were made into an orderly collection with no clear indication of how he felt towards the images:
Picture 2 was also at assessment, showing a clear ability to like, not like and feel unsure about aspects of self care.
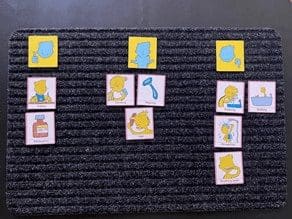
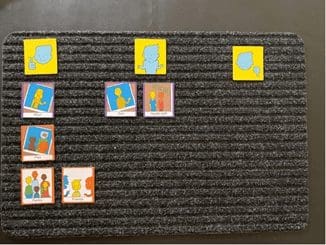
Picture 3 was during treatment for Psychosis and therapy – some changes were being noted with his self care and allowing his team to help him:
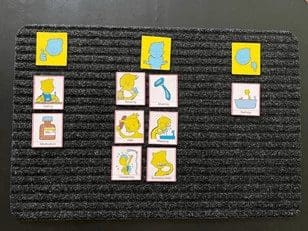
Picture 4 was towards the end of treatment and intensive therapy. Some aspects of bathing remained unsure, but his behaviour indicated that he was more comfortable with activities around bathing.
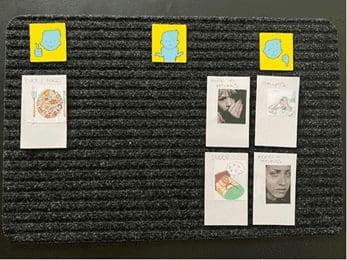
Picture 5 was a repeat of the family cards after treatment:
Picture 6 are the cards I have created based on the Mental State Examination – this was six months into therapy and medication. He expressed issues around his mood, thoughts and sleep – these needed more explaining. With the mood pictures, I offered my client different images for mood and he picked the ones that reflected what he was feeling. My mood collection has happy, angry, scared and sad in them as I tend to quote these 4 basic raw emotions daily in my work:
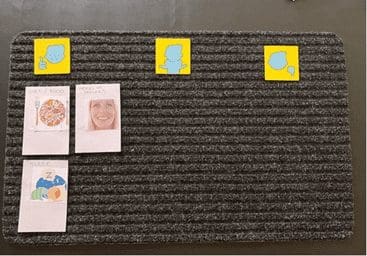
Picture 7 was at the end of treatment the same cards were used with a very different result. As for the previous mat, for the mood pictures, I offered my client different images for mood and he picked the ones that reflected what he was feeling:
Many thanks to Debbie Mole for sharing this powerful example. If you would like to read more about Talking Mats use in Mental Health, take a look at top 10 blogs here: https://www.talkingmats.com/top_10_mental_health/
If you are feeling inspired and have not yet accessed our Talking Mats Foundation Training Course, find out more here:
Many thanks to Karen Mellon, NHS Fife Lead Podiatrist for Learning Disabilities and Care Homes, for this guest blog describing our exciting Fife Health Charity funded project, aimed at supporting patients with a learning disability (LD), or dementia, to be more involved in decisions around their care.
I was initially introduced to Talking Mats by my Learning Disability SLT colleagues who were using the resource to support patient engagement. I could see the real benefits of how it could support our interactions with patients with a LD or dementia and empower people to be more involved with decisions around their care. Our SLT colleagues had undertaken the Talking Mats Train the Trainer program and were then able to train our podiatrists in using the resource. Having used the existing resources we found that we weren’t able to discuss/explore people’s views deeply enough, for example, when they developed a foot ulceration, or were at risk of ulceration. This was the spark that ignited the idea to look at developing a specific foot care resource to enable these conversations.
The aim was to promote patient engagement in their care – both in preventative care and when specialised input is required. By creating the resource we aimed to explore what really mattered to the person and what for them were acceptable goals and outcomes. By developing a specific Talking Mats resource we were able to explore treatments options and impact of conditions and actively engage the person in expressing their views thus creating a person centred care plan. Evidence shows us when people are involved in decision making they are more satisfied with their care, which in turns improves their quality of life.
Having consulted with Talking Mats we jointly created an initial resource which we piloted within NHS Fife over a 6 week period. People living within care homes and people with a learning disability were the target audience for the pilot. Using the resource, we were able to understand more about the impact that foot ulceration was having on patients, and patient’s views on treatment options.
One example of this positive impact involves a 60 year old patient with learning disabilities and dementia. She lives independently with one hour support each day to assist with personal care. She has been known to podiatry for some time due to repeated ulceration. Specialist footwear has been supplied and regular input is in place to reduce the risk of re-occurrence, however at times the foot does break down.
In May the patient experienced a break down on her foot. She is a very pleasant lady who always comes across as if nothing bothers her and everything is fine; she doesn’t like to “cause a fuss”. It was felt the use of a Talking Mat might give us greater insight into the impact the wound was having.
As a result of completing the Talking Mat we were able to discover the patient was in fact experiencing difficulties with the type of dressing and was experiencing pain. We were able to address this and change the dressing type to an adhesive dressing, which took up less room in her shoe, and started her on Paracetamol 4 times a day to address her pain. Follow up discussions reveal the patient was much more satisfied with the dressing, it was more comfortable and easier to keep dry when showering. She also reported to be experiencing much less pain.
As a result of the mat, we were able to identify concerns she had, but didn’t want to share as she didn’t want to be a burden. We were able to address this and create a plan which was acceptable to the patient and improved her wellbeing.
I hope this resource will go on to benefit other professionals and carers working with people who may be impacted by their foot health. By using this resource, we can help our patients explore their views and wishes, therefore enabling co-production in care. The resource promotes preventative care as well as specialist intervention. Going forward there are many other areas of foot health that could potentially be explored in developing further resources – such as paediatrics, nail surgery, musculoskeletal.
Book your place on the Talking Mats and foot care training course on 24th January 2024 / 21st February 2024 being run jointly between ourselves and Karen Mellon . The price includes the resource .
To find out more about the work and projects supported by the Fife Health Charity follow their Social Media accounts at:
Facebook – @fifehealthcharity
Twitter – @FifeHealth


